Redo TAVR: Clinical Evidence

05/22/2023
Daily practice and recent updates in the guidelines have made transcatheter aortic valve replacement (TAVR) a first-line treatment option for younger patients with lower surgical risk.1-4 As a result, it is estimated that the life expectancy of many TAVR patients will exceed the durability of their bioprosthetic valve; in many, a redo TAVR (ie, valve-in-valve in the failed transcatheter aortic valve [TAV]) may be indicated. Although valve-in-valve has become fairly common for failed surgical tissue valves, redo TAVR can potentially bid a new outline of challenges and outcomes. This article reviews key points concerning this new outline based on contemporary clinical evidence.
PATIENT CHARACTERISTICS AND PRESENTATION TO REDO tavr
Early data regarding patient characteristics were published by Barbanti et al in 2016.5 In this registry, the redo TAVR prevalence was 0.4% of the overall TAVR volume, and the main redo TAVR indication was moderate or severe paravalvular aortic regurgitation (PVR; 50%) or central regurgitation (28.3%). The mean time interval between the index and redo TAVR was 812 ± 750 days, and patients presented with New York Heart Association (NYHA) functional class III or IV dyspnea (72%) or in acute heart failure (14%). The time to valve failure was significantly shorter in patients presenting with PVR compared to those presenting with stenosis or central regurgitation (ie, suspected structural valve degeneration: 435 ± 594 vs 1,189 ± 706 days).5 These findings most likely reflect a more rapid clinical deterioration in cases of procedural-related valve failure (resulting from TAV malpositioning, sizing error, or asymmetrical frame expansion) as compared to primary/inherent TAV-related failure (resulting from structural valve degeneration, thrombosis, previous endocarditis, or a combination of those).
These differences in TAV failure mechanisms were further addressed in the Redo-TAVR registry.6 In this study, patients were classified as “procedural failure” if they presented within 1 year of the index TAVR or as “TAV failure” if they presented beyond 1 year of their index TAVR. The median time interval to redo was 5 (range, 3-6) years among patients with probable TAV failure, compared to only 68 (range, 38-154) days among patients with probable procedural failure. TAV failure phenotype was different in patients with probable procedural failure compared to those with probable TAV failure. Dominant aortic regurgitation (AR) was more frequent in the first cohort (73% vs 29.7%; P < .001), whereas dominant aortic stenosis (AS) was more common in the latter (16.2% vs 37%; P = .002). A main limitation of this study was that data on AR location (PVR vs central AR) were not available.
In the TRANSIT registry, redo TAVR constituted 0.44% of the TAVR population. Again, the primary indication for redo was AR (56%) followed by AS (33%) or combined AS/AR (11%).7 Patients almost invariably presented with advanced symptoms (NYHA class III/IV in 73.5%).7 In this study, the mean index-to–redo TAVR time was 362 ± 337.8 days for the Portico valve (Abbott) and 1,343 ± 1,056.1 days for the Sapien valve (Edwards Lifesciences). Patients with self-expandable valves (SEVs) presented earlier than those with balloon-expandable valves (BEVs), yet again TAV failure etiology likely resulted from both procedural and “primary” TAV failure.7
PROCEDURAL SUCCESS, COMPLICATIONS, AND MORTALITY
Due to a large diversity in patients’ aortic root anatomies, TAV stents configurations, leaflet positions, and deployment depths of the index TAV, redo TAVR can be technically challenging. Figure 1 illustrates the main outcomes according to the largest series to date.5-8 Early data show acceptable rates of acute complications (2% stroke, 2% coronary occlusion, and 2% valve embolization), apparently acceptable acute valve performances (high residual gradients [> 20 mm Hg] in 10% of cases), no in-hospital mortality, and 85% survival at median follow-up of 586 (range, 8-2,460) days.5 Procedural success was reported to be fairly similar in the TRANSIT (79%) and Redo-TAVR (85%) registries.6,7 In both studies, procedural failure was mostly related to valve malperformance with residual high gradients in 14% and AR > +1 in 7% to 9%. The rate of periprocedural complications was comparable with 3.5% strokes and 9.6% new pacemakers implantations, as was mortality at 30 days and 1 year with 3% and 13.5% in the Redo-TAVR registry and 7% and 10% in the TRANSIT registry, respectively.6,7
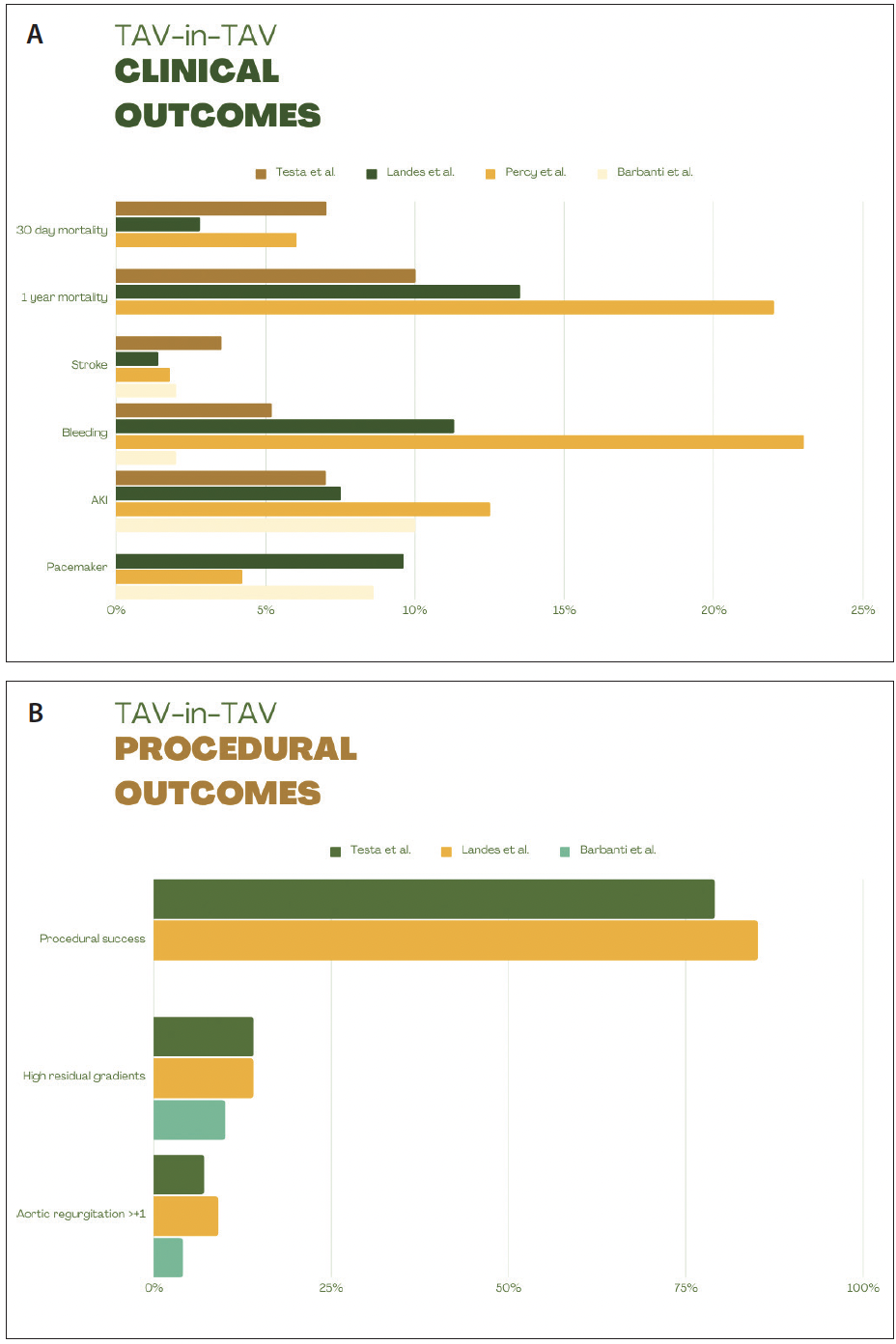{kind=link}
When redo TAVR was compared to TAVR-in–surgical aortic valve (SAV) using propensity matching, mortality was similar at 30 days (3% vs 4.4%; P = .556) and 1 year (11.9% vs 10.2%; P = .663); yet TAV-in-TAV was associated with higher procedural success compared with TAV-in-SAV (72.7% vs 62.4%; P = .045) driven by a lower proportion of patients with residual high gradient (14.6% vs 21.5%; P = .095).9 Similar findings were reported by Raschpichler et al who found better hemodynamics after TAV-in-TAV versus TAV-in-SAV (median prosthesis mean gradient: 12.5 mm Hg [IQR, 8.8-16.2] vs 16 mm Hg [IQR, 13-20.5]; P = .045).10 The larger internal diameter and the lack of a rigid sewing ring in TAVs can probably explain these more favorable hemodynamic results compared to SAVs.
In a more recent publication, redo TAVR outcomes were assessed according to the type of the initial and subsequent valve: either BEV or SEV.11 In this study, there was no association between TAV type (either index or redo) and mortality or procedure safety. On the other hand, patients with BEV presented later than SEV (4.9 ± 2.1 vs 3.7 ± 2.3 years after TAVR; P < .001) and device success was higher when SEV (vs BEV) was used in the redo TAVR (77.2% vs 64.3%; P = .045), primarily because of lower residual gradients.11 In further analysis, TAV deployment depth (second TAV relative to the index TAV) was measured using the post–redo TAVR fluoroscopic images.12 Deployments were classified as “conventional” or “unconventional,” based on depth scattering inside or outside the IQR (25th to 75th percentiles) of a patient’s respective subgroup (BEV-in-BEV, SEV-in-SEV, BEV-in-SEV, and SEV-in-BEV). Although the number of acute procedural complications was low, all of them occurred in the “unconventional” depth cohort and translated into higher mortality rate in this cohort (0% vs 8.1%; P = .021).12
Up-to-date clinical experience sets redo TAVR as a key strategy to treat failed TAVs, especially when considering the relatively higher risk associated with alternative options such as surgery and TAV explantation or conservative management. In the EXPLANT-TAVR study, in-hospital mortality was 11.9%, 30-day mortality was 13.1%, and 1-year mortality was 28.5%.13 In an analysis based on the Medicare and Medicaid registry, TAVR explantation was associated with higher mortality compared with redo TAVR (12.3% vs 6.2% at 30 days; P = .05) as well as higher in-hospital bleeding (odds ratio [OR], 2.6), acute kidney injury (OR, 2.14), and longer hospital stay (6 vs 10 days).8 Importantly, endocarditis was the main indication for explantation (43%) and grants a strong bias that can explain at least some of the differences in outcome.13 On the other hand, TAV explantation surgery is a complex procedure that commonly involves root replacement (12.9%) or enlargement (7.1%).13
CORONARY OBSTRUCTION
Coronary obstruction (CO) is a relatively rare but catastrophic complication related to any TAVR procedure.14 CO during TAVR in native AS is extremely rare and primarily relates to the displacement of the calcified native leaflets against the coronary ostia. The rate of CO during TAV-in-SAV is higher due to the dislodgment of the bioprosthetic valve leaflets toward the coronary ostium as a consequence of TAV stent expansion. Based on the VIVID registry, the rate of CO during TAV-in-SAV is 3.5%.15 In redo TAVR, the theoretical CO risk appears to be even higher due to the creation of a “neoskirt” when the leaflets of the index TAV are pinned open by the redo TAV.16 This neoskirt may cause sinus of Valsalva sequestration if the top end of the skirt reaches the level of the sinotubular junction (STJ) while in contact with the aorta, hence obstructing blood flow to the sinuses. Although CO was infrequent both in the Redo-TAVR (1.2%) and TRANSIT (no events) registries, it is imperative to remember that patients in those studies were highly selected and deemed anatomically suitable for redo TAVR. We do not know how many were denied redo TAVR due to anatomic concerns.
Because there are only a few bailout strategies to manage CO once it occurs (such as “chimney” stenting or emergent bypass surgery) and none are ideal, prevention is essential. With the help of the CT scan, one can place a virtual redo TAV inside the index TAV and measure various TAV-to-aorta reserves, such as the valve-to-coronary and valve-to-STJ distances.17 BASILICA (bioprosthetic or native aortic scallop intentional laceration to prevent coronary artery obstruction) is a transcatheter splaying of the aortic valve leaflets, potentially reducing the risk for obstruction.18 In the BASILICA trial, BASILICA was successful in 95% of attempted leaflets with 100% freedom from CO and reintervention in SAVs. However, BASILICA is an extremely complex procedure, and in 30 days, there were 3% disabling strokes and 7% nondisabling strokes.19 Moreover, BASILICA is potentially less effective in TAVs compared to SAVs as transcatheter valve deployment so far does not systematically allow valve-to-coronary alignment and also the leaflets can get pinned between the failed TAV and the new TAV frames and fail to splay and allow coronary perfusion.20 Bench testing suggests that newer-generation TAVs (Sapien 3 and Evolut [Medtronic]) demonstrate less effective splay, and in the case of Evolut, adequate splay is achieved only high above the base of the leaflets,21 making some suggest balloon assisted–BASILICA to be potentially more effective (where a balloon is inflated across the leaflet prior to the laceration, increasing the leaflet splay).22,23 Dedicated devices for leaflet laceration are also in the pipeline and are expected to improve the utility of these procedures. Recently, a first-in-human results of the ShortCut device (Pi-Cardia) showed feasibility and good success rate.24
FUTURE CORONARY ACCESS
Coronary artery disease is prevalent in TAVR patients, and coronary access after redo TAVR is also a key factor to consider. The post–redo TAVR aortic root can be challenging for catheter navigation and crossing, especially if the distance from the index TAV and the aortic wall is small (< 2 mm, which is the minimal space needed when using a 6-F catheter).16 Another possible obstacle can be the misalignment between the first and second stent struts that can make catheter cannulation extremely hard or even impossible. In a study by De Backer et al, 45 post–redo TAVR CT scans were analyzed to examine coronary accessibility, divided into four subgroups depending on their valve’s configuration.25 The neoskirt was taller in patients with index TAV who had tall frame and supra-annular leaflets; 90% of these patients had coronary ostia below the top of the neoskirt compared to 67% in patients with index TAV with short frame and intra-annular leaflets.25 Shorter TAV-to–aortic wall distance and strut misalignment were also factors to consider and more prevalent in patients with index supra-annular SEV.25 In a prospective study by Nai Fovino et al, 137 TAV-in-TAV patients underwent coronary angiography. Coronary access was classified as feasible if the coronary ostia was above the top of the neoskirt, theoretically feasible if the coronary ostia was below the top of the neoskirt yet the distance from the TAV frame and the aortic wall was > 2 mm, and unfeasible in cases where that distance was < 2 mm. Coronary access was found to be feasible, theoretically feasible, and unfeasible in 40.9%, 27.7%, and 31.4% of the cases, respectively. Independent predictors for impaired coronary access were supra-annular index TAV (OR, 6.61; P = .002), smaller STJ diameter (OR, 0.62; P < .001), and female sex (OR, 3.99; P = .04).26
FUTURE EVIDENCE
Current evidence provides overall reassuring data on the outcomes of redo TAVR; however, all studies so far have been retrospective and included highly selected patients and relatively early reinterventions for multiple indications beyond structural valve degeneration. As more robust data are required and because randomized trials are unlikely to be applicable soon, efforts are being made to develop large prospective registries. Such a registry (NCT05601453) is planned to include approximately 200 patients who will undergo redo TAVR with the Sapien 3/Ultra in 50 European centers. Patients who will be managed conservatively or undergo surgical explantation will also be included in parallel registries.27 The REVALVE registry is planned to include 300 to 500 patients in the main redo TAVR arm as well as surgical explantation and conservative management parallel arms in 75 to 100 centers across Europe with up to 5-year follow-up.27 Until more clinical data become available, redo TAVR practice will lean on expert opinions and theoretical concerns (Figure 2) and should always involve a multidisciplinary team.
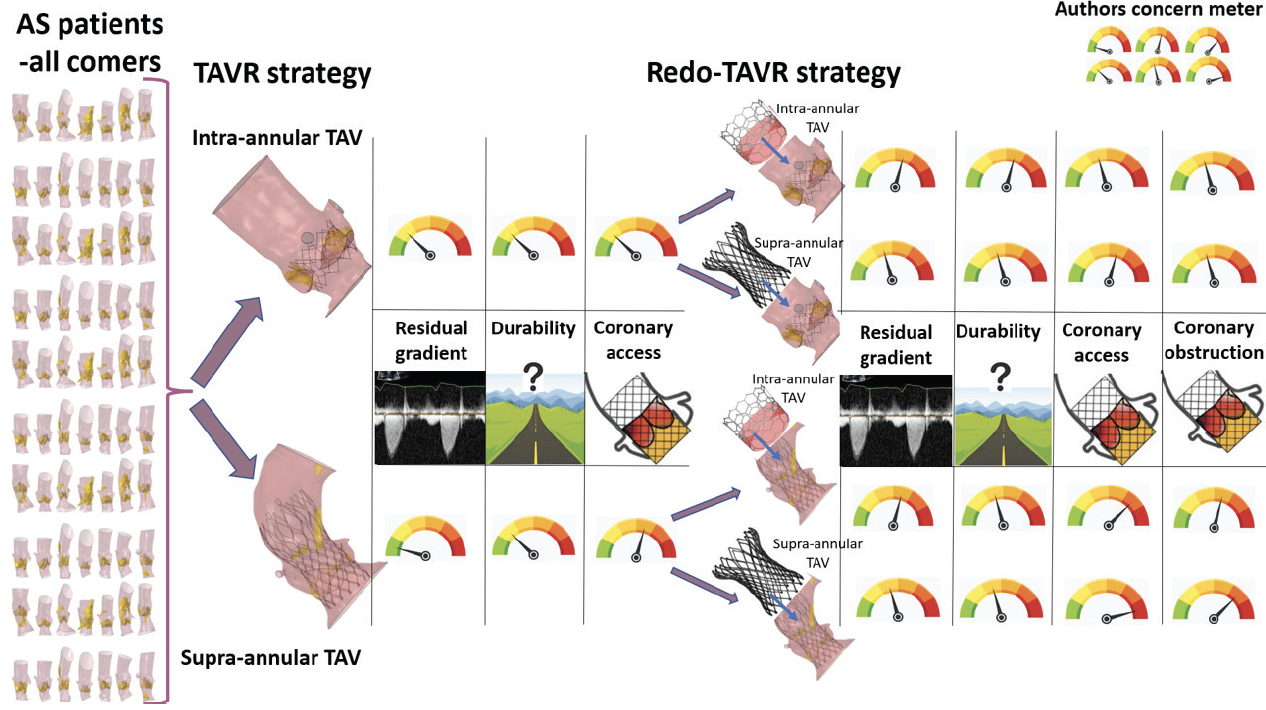{kind=link}
Figure 2. This figure illustrates the personal level of concern regarding particular topics that surround redo TAVR in a generic patient population. This is not at all applicable/deductible for a particular patient, where the native aortic root anatomy or valve position can cast out a totally different profile of concerns.
CONCLUSION
Based on the ongoing clinical data regarding valve durability, procedural success, and low complication rate and the current trends toward minimally invasive strategies, TAVR will expand to include younger patients with longer life expectancy, and redo TAVR will be more frequently needed. This revolution will require more strategic thinking when planning the primary procedure. This long-term planning and decision-making should involve a multidisciplinary team of interventional cardiologists, cardiac imagers (CT and echocardiography), and cardiac surgeons, as well as the patient.
Ady Orbach, MD, MSc
Attending Cardiologist
Wolfson Medical Center
Holon, Israel
Disclosures: None.
Uri Landes, MD
Wolfson Medical Center
Holon, Israel
uri.landes@gmail.com
@LandesUri
Disclosures: None.
Facebook Comments